Pubmed citation
Full Paper
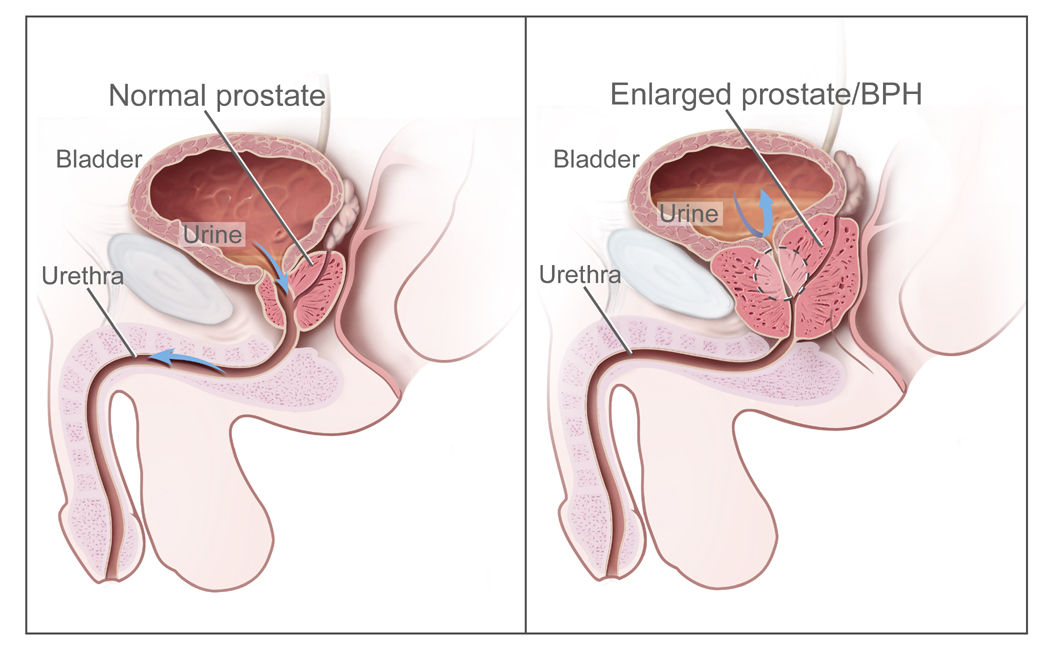
The paper deals with laser prostate surgery for benign prostatic hyperplasia (BPH), commonly known as an enlarged prostate.
Our experience with the procedure reveals that it is safe to perform this surgery with a discharge within hours of the procedure. This case series is important because having an ambulatory pathway can reduce hospital resource utilization, allow patients a more comfortable recovery in their home environment, and avoid further exposure to hospital based problems such as infections, errors, and falls.
In a laser prostatectomy, a laser fiber is used to destroy prostate tissue that is blocking a man's urinary flow. An advantage from a laser based approach is less blood loss due to the sealing action of the laser. This allows patients the potential for a same day surgery.
The classic, surgical approach to BPH is the TURP or transurethral resection of the prostate. As a opposed to a laser fiber, a cutting loop is used to shave away the obstructive prostate tissue. Due the amount of bleeding postoperatively, patients are generally admitted to the hospital for at least one day with a bladder irrigating catheter.
Our research group is currently studying other aspects of advanced laser prostate surgery as well as the use of mobile apps in urology....so stay tuned! More abstracts and papers to come...